
ECG Basics
WHAT DO PQRST WAVES REPRESENT ON AN ECG?
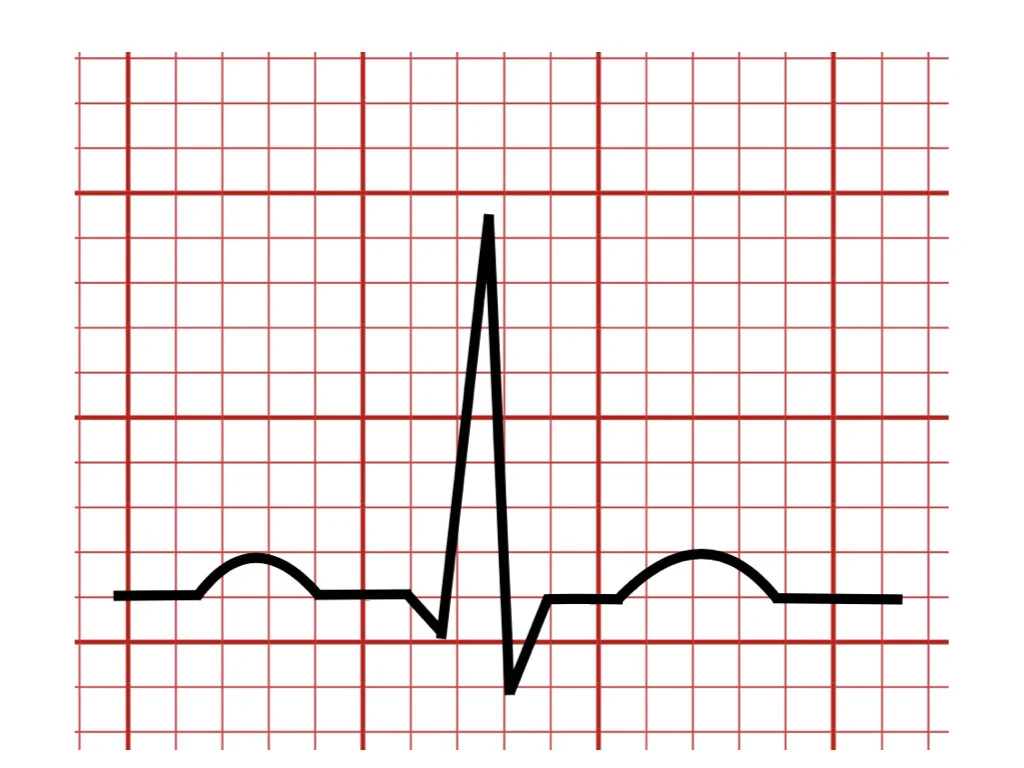
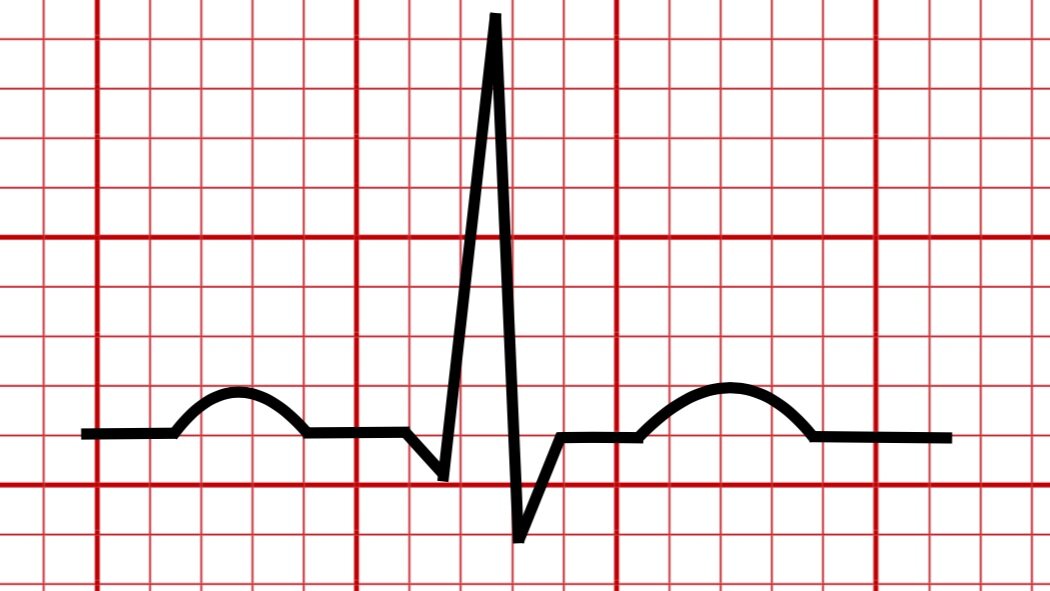
In this article, you’re going to learn the basic meaning of the P-QRS-T waves. This will be a simplified overview of this topic. In later articles, I’ll review each wave independently more in-depth.
But first, let’s understand two important concepts that dictate the electrical conduction of the heart :
•Depolarization – Refers to the loss of negative charges inside the myocardial cell.
•Repolarization – Refers to the gain of negative charges inside the cell with the resumption of its initial resting state.
Both depolarization and repolarization of the cardiac cells form the basis of the electrical conduction in the heart that excites the contraction of the atrial and ventricular chambers.
•P wave – Represents the Atrial depolarization
•QRS wave – Represent the Ventricular depolarization
•T wave – Represents the Ventricular repolarization

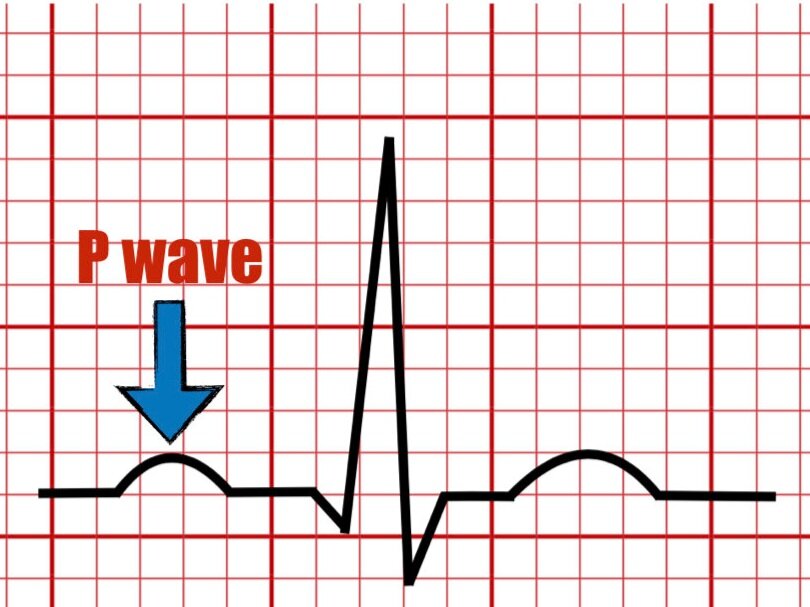
The P wave is the first wave in the normal ECG tracing (assuming sinus rhythm is present) that represents the electric current originated from the SA node that travels along the right and left atrial chambers signaling atrial contraction thus transferring blood into the ventricles.
The P wave is mostly positive in leads I and II and is biphasic in leads V1 and V2 with a varying axis ranging from 0 to + 75 degrees.

P wave as seen normally in lead II
Two atrial components of a positive P wave commonly seen in lead II
The P wave can be divided into the right and left components that represent depolarization of the right and left atrium.
There are normal parameters for both the size and duration of the P wave. Any value above the limit of normal could be indicative of atrial chamber enlargement.
The atrial repolarization is usually embedded inside the QRS complex and is not seen on the surface ECG given its low amplitude.
CLINICAL CORRELATION
Occasionally the ECG lacks the P wave and may demonstrate an irregular rhythm. In these cases, a thorough evaluation of the P wave is warranted to exclude the possibility of a very common rhythm abnormality called atrial fibrillation which can lead to stroke among other serious consequences.
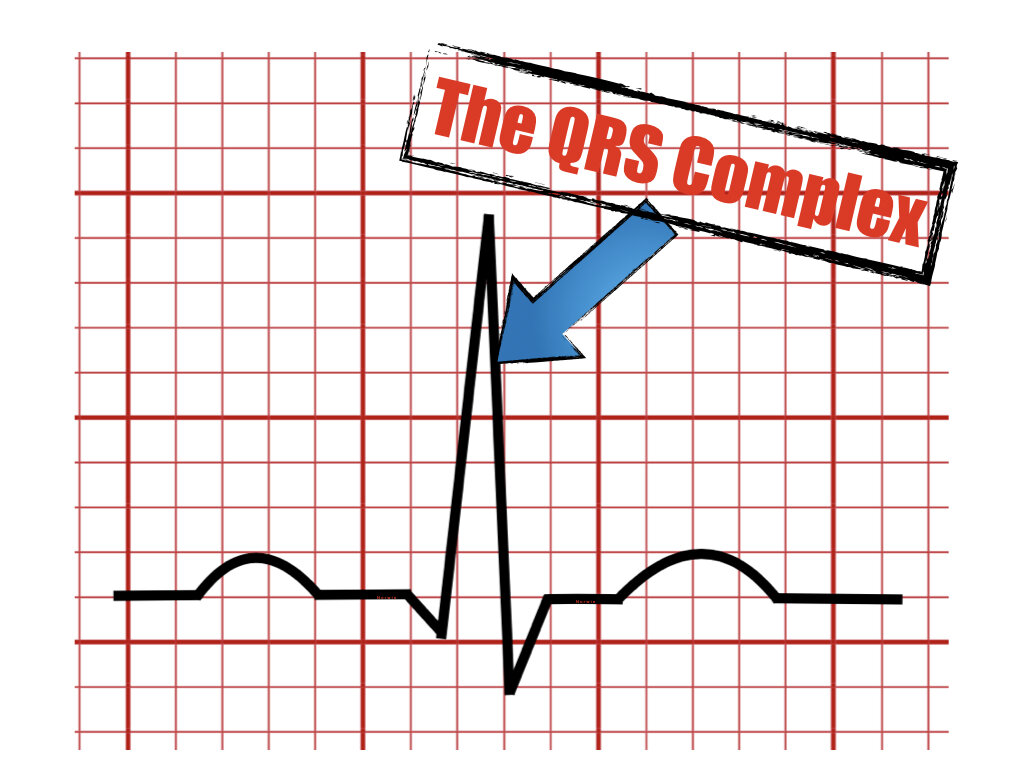
THE QRS COMPLEX

The QRS complex
The QRS complex reflects the ventricular activation or the electrical current that runs along the ventricles and stimulates ventricular contraction which will eject blood out of the heart to reach other vital organs.
The QRS is divided into the Q, R, and S waves.
•The Q wave is the first negative deflection after the P wave and can be seen in normal patients but can also suggest scar tissue of prior myocardial infarction depending on the size, duration, and localization of the wave.
•The R wave is the first positive deflection after the Q wave. Changes in the size out of the normal values can be seen in many cardiac abnormalities.
•The S wave is the first negative deflection after the R waves and is deepest in the right precordial leads. It is often absent in leads V5 and V6.
Similarly to the P wave, any variation in the size and duration of the QRS complex out of its normal values could be a normal finding or indicative of a cardiac abnormality.
When comparing the size of the P wave with that of the QRS complex, it is evident their size discrepancies which are due to the larger size of the ventricles producing a higher voltage versus the smaller atriums which produce a lower voltage on the ECG.
Finally, it is important to know there exist additional QRS complex morphologies including the RS, R, rSR, RSR’, QS that I will elaborate on in another article to avoid confusion.
CLINICAL CORRELATION
Clinical states associated with altered QRS complex parameters of both size or duration may include but are not limited to:
•Enlargement of the ventricular muscle (hypertrophy)
•Pericardial effusion
•Cardiac tamponade
•Prior myocardial infarction
•Electrical conduction disease
•Infiltrative disorders of the heart
•Endocrinologic problems (i.e, hypothyroidism)
THE T WAVE

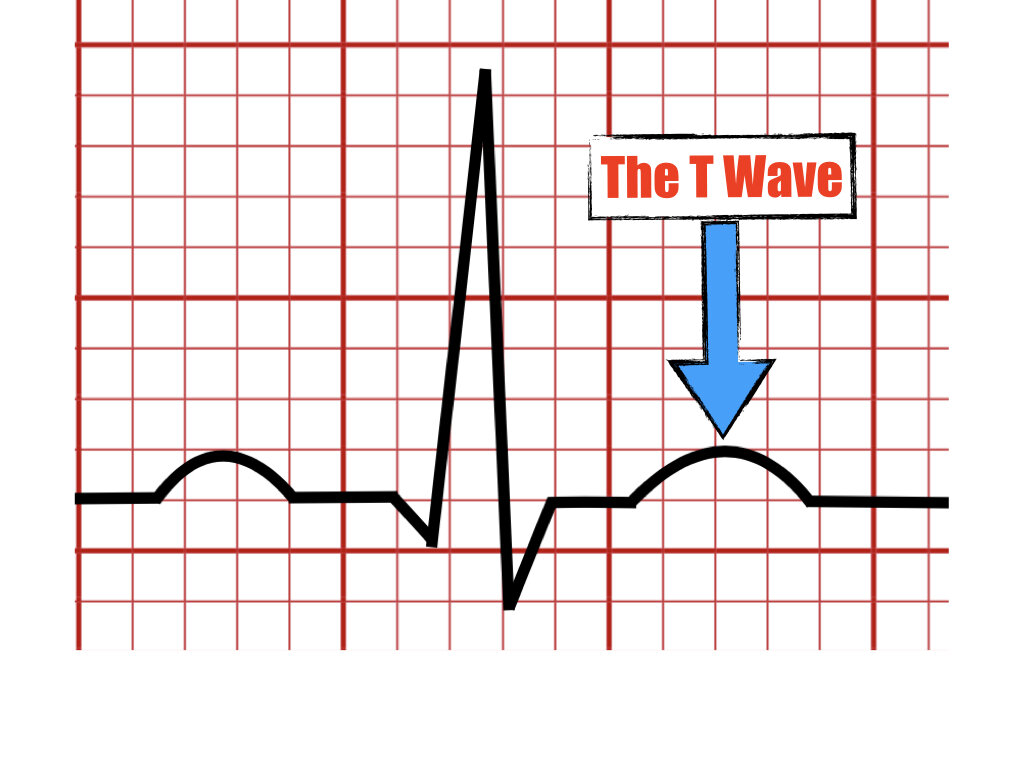
The T wave
The T wave is the last wave seen after the QRS complex and represents the ventricular repolarization (restored negative electrical charges inside the ventricular cells).
T waves are always upright in leads I and II and inverted in lead aVR and their amplitude is usually < 6 mm in limb leads and ≤ 10 mm in the precordial leads.
The T wave can have different morphologies including upright, peaked, notched, biphasic, or inverted.
Abnormalities in the size and shape of the T wave can be seen during electrolyte disturbance such as abnormal levels of potassium. Also, a poor supply of oxygenated blood to important regions of the heart may lead to significant T wave changes.
T wave inversion located in the right precordial leads can be a normal finding in young individuals this is known as juvenile T waves but T wave inversion in the right precordial leads is relatively uncommon in adults. Hence, for this reason, it is always important to correlate the age and the clinical presentation of the patient when analyzing ECG findings to avoid errors of interpretation.
Occasionally a U wave can follow the T wave and is believed to represent late phases of the ventricular repolarization.
KEY TAKEAWAYS
•Depolarization and repolarization form the basis of the electrical conduction of the heart.
•The P wave is the first wave and represents atrial depolarization leading to atrial contraction.
•The QRS complex represents the ventricular depolarization resulting in ventricular contraction.
•Atrial repolarization is embedded inside the QRS complex and is not visible.
•The T wave is the last and represents ventricular repolarization.
REFERENCES
•Surawicz, B., Knilans, T. K., & Chou, T.-C. (2008). Chou's electrocardiography in clinical practice: Adult and pediatric. Philadelphia, PA: Saunders/Elsevier.
•Zipes D, Libby P, Bonow R et.al, Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine 11th edition, 2018
•O’Keefe J, Hammill S, Freed M, The Complete Guide of ECGs 4th edition, 2016
Please send your feedback !
In this blog, we are going to explain the meaning of the U wave in the electrocardiogram and provide examples of normal and pathologic causes of its appearance on the ECG.